- Discover how we are helping Members reduce emissions: Explore the ProjectGHG hub now.
- Join the global DP Community at the IMCA DP Conference in Amsterdam. 21 and 22 May. Book now
- Register your interest for the IMCA Global Summit 2024. 3-4 December, Utrecht, Netherlands.
- Now booking. Underwater Ship Husbandry Seminar. 10 October 2024, Singapore.
Near miss: dropped clump weight
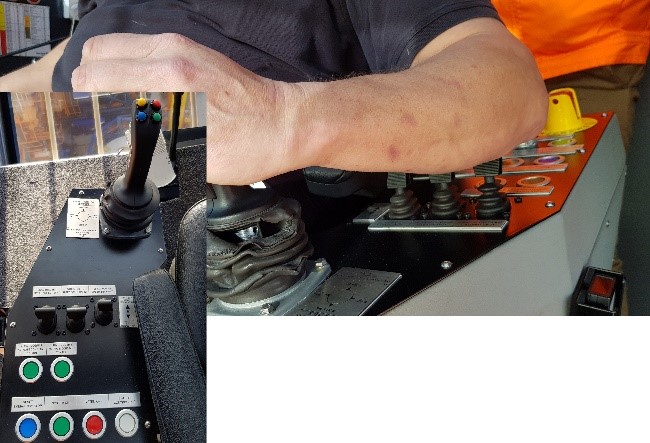
What happened?
A clump weight fell approximately 30m to deck and landed around a metre to where a rigger was working. The incident occurred just after the boom of the main crane was lowered towards the cradle for sea fastening prior to transit. It was dark, windy and raining. The crane operator stopped lowering the boom to verify using the camera that the boom was in the correct position. As the camera view was blurred by rain and glare from the lights, the operator leaned forward to look at the boom. At that moment, his elbow unintentionally touched the tugger winch lever. The tugger winch started pulling on the tugger wire and pulled the rigging onto the sheave in the boom. Since a wedge socket was part of the rigging, the wedge was pushed down when the wedge socket hit the sheave, releasing the tension on the wire. As a result, the wire was pulled out of the wedge socket. The wedge socket, shackle and clump weight dropped 30m to the deck and landed one meter from where a rigger was working.
What were the causes?
- No safeguards in place to prevent unintentional activation of the tugger winch by operator;
- No mechanisms in place to stop rigging being pulled onto the sheave;
- A wedge socket was recently introduced into the rigging configuration (changed from original spelter socket);
- The lever of the tugger winch was installed as per design, positioned close to the elbow.
What lessons were learned?
- Relying on certification of the crane does not guarantee that the crane is intrinsically safe by design. A certified crane also has residual risks that should be evaluated with a risk assessment;
- Unintentional activation of control levers should be evaluated in a risk assessment;
- Changes to the design should be controlled with the management of change (MoC) process. This process should also focus on new risks introduced with the changes;
- Suspended objects have a risk of falling, although the risk might be small, the potential impact is severe.
What actions were taken?
- Verify if controls can be activated unintentionally and consider what would be the possible (worst) consequence;
- Evaluate if there are mechanisms in place to stop equipment from making contact e.g. limit switches;
- Consider what the weakest component is in the equipment configuration and what the consequence might be when it fails.

Members may wish to refer to:
Safety Event
Published: 28 April 2020
Download: ![]() IMCA SF 14/20
IMCA SF 14/20
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.