MOB fatality from multi-cat

What happened?
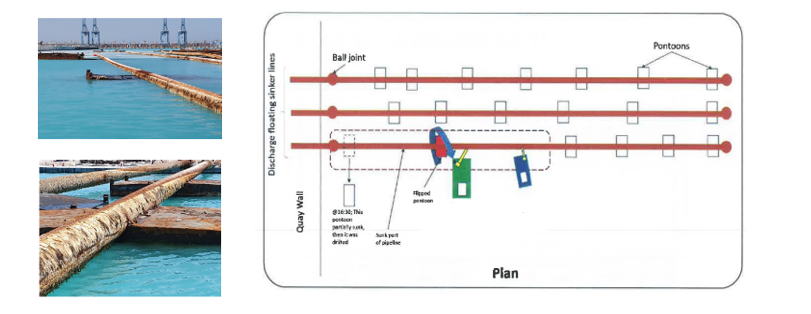
A member reports a man overboard fatality which occurred from a multi-cat engaged in shallow water construction in an inshore environment. The task involved recovery and re-arrangement of a pipeline configuration, consisting of 3 x 300m sinker-pipe, which was connected to shore using 7 floating pontoons. Three separate pipes were used for dewatering a reclamation site. One of the pipes including pontoons was partly submerged. The operation took place in low light conditions during the hours of darkness
The initial plan was to re-float the pipeline with a technique using compressed air. Whilst the task was ongoing, there was a change to the plan, and it was decided to lift the floating pipeline configuration using the crane on the multi-cat. As the lift started, one of the floating pontoons flipped over the pipeline and hit the Chief Engineer who was operating the crane, causing him to fall overboard. Immediately an AB on deck jumped overboard to help him; the Chief Engineer was recovered and first aid /CPR undertaken. He was transferred to hospital but was unfortunately declared dead later that evening.
What went wrong?
During the operations, the decision was made on-site to change the plan and use the deck crane of the multi-cat to lift the pipe-line and use another workboat to place a pontoon underneath. One of the pontoons was not secured to the pipeline; this came loose, surfaced and flipped over the floating pipeline, hitting the multi-cat crane and the Chief Engineer, who was driving the crane.
- There was an unplanned change, from using the air compressor to lifting the pipeline using the multi-cat crane;
- There was no risk assessment nor Management of Change (MoC) process applied to the changed plan;
What were the causes?
Our members’ investigation identified the following root causes:
- Inadequate worksite supervision
- Site supervisor ignored the instructions to postpone the operations after the first attempt to follow the initial plan. He changed the plan, without following the appropriate MoC process;
- Operations were conducted in hours of darkness, against company instructions;
- Unsafe Lifting Operations
- The sunken dewatering-line was lifted using the Multi-Cat deck crane;
- Lack of Situational Awareness
- There was no adequate (risk) assessment of the job or work area;
- No-one involved recognized the hazardous situations and did not use STOP WORK authority.
Members may wish to refer to
- SEL 035 In the line of fire video
Safety Event
Published: 13 July 2020
Download: ![]() IMCA SF 21/20
IMCA SF 21/20
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.