Lost time injury (LTI): Dropped object incident
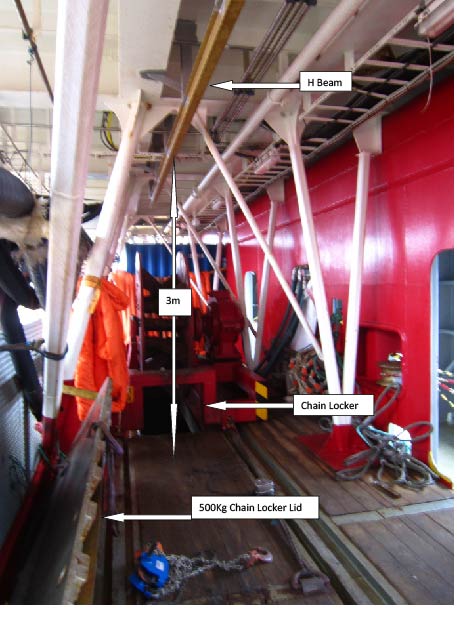
A member has reported an incident in which someone sustained a serious neck injury as a result of a dropped object incident. The incident occurred whilst members of the crew were using a chain block/tackle assembly on a H-beam, to assist with manoeuvring the heavy lids to the chain lockers which were located on a mezzanine deck. As chain locker lids are too heavy to move manually, two months previously, an H-beam had been installed in this location to permit the use of a chain assembly/trolley.
One of the persons conducting the work manually pulled the chain aside; momentum caused the trolley for the chain block assembly to run along the H-beam track. There was no end stopper and the trolley fell off the H-beam. It fell approximately 1.2 meters, glancing off the injured person’s helmet and landing on deck. The total weight of the trolley and chain block assembly was approximately 33 kg. The injured person walked off the job unaided, and was attended by the onboard medic. The initial prognosis was a fractured neck. A neck brace was applied and then the injured party was medivaced by helicopter.


Our member’s initial investigation noted the following immediate causes:
- There was no ‘trolley stopper’, or similar device, on the H-beam, to prevent chain assembly/trolley from falling off the end of the beam;
- The injured person was working under a unsecured load and ostensibly unaware of the consequences of pulling the chain assembly along H-beam when there was no trolley stopper;
- The injured person disconnected the chain from chain locker lid.
Our member noted the following root causes to the incident:
- Organisation
- Although there were four persons working on the particular job, there was a lack of supervision, as work instructions were not followed;
- Work equipment was allowed to be used, despite being known and identified as ‘faulty’. The day before the incident it had been reported that there was no ‘trolley stopper’ on the retrofitted H-beam. No action was taken to address this very serious omission;
- The potential of falling objects was not recognised or identified as a foreseeable and significant risk. . People -Work instructions were not followed. The injured person disconnected chain from chain locker lid; this was not a specified work instruction within documentation, nor instruction from the lead AB. The injured person appeared to have been working from his own initiative in undertaking this action. . Environment -There was a lack of situational awareness. The injured person and his colleagues, whilst familiar with the generic activity of opening chain locker doors, were not familiar with the new H-beam and the overhead chain assembly tool and this may have contributed to the incident occuring. It was noted that this was the first time the H-beam/chain assembly tool arrangement had been used at this worksite.
Our member took the following actions:
- Installed a trolley stopper on that particular H-beam;
- A fleet-wide ‘time out for safety’ was carried out, and further DROPS awareness training was organised;
- A DROPS survey was performed with all similar beams inspected and maintained at member worksites;
- Checked certifications of H-beam, lifting equipment and chain assembly requested for inspection.
Members’ attention is drawn to the following IMCA material which may be of assistance:
- Avoiding dropped objects (poster)
- Avoiding dropped objects (pocket card)
Safety Event
Published: 23 September 2013
Download: ![]() IMCA SF 15/13
IMCA SF 15/13
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.