Closed bus common cause
- DP Event
- Published on 13 April 2022
- Generated on 27 June 2026
- DPE 01/22
- 4 minute read
Incident
The engines on standby auto started... It was apparent that all running engines were slowing down to the point they stopped.
Overview
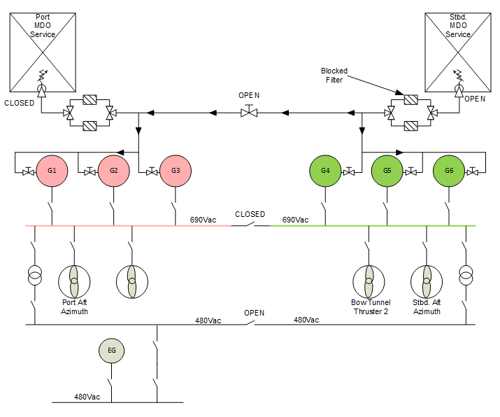
A DP2 ROV Support Vessel was conducting a pipe survey in open water. As the consequence of loss of position was considered low, it was decided to close the bus ties to minimise the number of connected generators. At the same time, the technical staff wanted to open up and inspect one of the fuel service tanks. The vessel had suffered fuel contamination with water throughout the fuel system which caused a build-up of sludge affecting the fuel filters.
The technical department was given approval to common up (cross connect) the fuel supply system to a single service tank from the starboard redundancy group. The port service tank was emptied and opened ready for inspection and cleaning. After 48hrs configured in this way, it was noted that there was the odd frequency alarm being reported on the vessels management system. Three out of the six generators were connected with the load on each generator between 60-65%.
At around midday of the third day, the weather had increased slightly, and engine loading increased. Another generator was started and connected. Once connected, bus frequency alarms were activated and didn’t clear. The frequency continued to fall to the level where all generator incomer breakers tripped along with the bus tie on under frequency and blacked out the vessel. The engines on standby auto started. It was apparent that all running engines were slowing down to the point they stopped.
The emergency generator started and connected to the emergency switchboard. The bridge was informed of the situation. The vessel was left without propulsion drifting in open water. The ROV crew made provision for the ROV. The technical department immediately identified that the fuel supply filters were the immediate issue and changed them to the clean set-in order to restore a supply to the engines. In the meantime, the blocked set were being cleaned.
Several attempts were made to start an engine however, it wasn’t until the governor was reset that the engine was able to start and be connected to the dead bus. Gradually, the vessel systems were brought back online and full power was restored.
It was decided to monitor the filters and change onto a clean set every hour. The port service tank was sealed and filled with clean fuel. Once filled and with the bus ties closed, the port engines were stopped. The fuel system was split, and the port engines were started and connected to the common bus. Once all checks had been made and the technical staff were happy, the bus tie was opened. The vessel was now on two independent redundancy systems.
What can be concluded?
- The vessel was working in ‘Task Activity Mode’ (TAM) which allowed for the risks associated with closed bus operation. The ASOG accounted for TAM.
- The jeopardy was cross connecting the fuel system and removing the redundancy of supply by isolating the port service tank for inspection and cleaning.
- Even in open water, care must be taken in assessing the risks. This vessel was fortunate that it did manage to recover without any significant effect on human safety or asset damage. However, if the incident had been prolonged, the comfort of the crew with regards to the vessel’s sea keeping ability, would have been affected.
- What started out as a good idea to take advantage of the open water low consequence effects soon rapidly turned into a much degraded and a potentially dangerous situation.
- It was unclear if the auxiliary system configurations were included within the ASOG. If they were not considered, then this event clearly shows that they should be taken into account.
- The implications of contaminated fuel in the system were not fully understood.
- Were the full blackout recovery drills training adequate and effective? The vessel did recover but could there be room for improvement?
Latest DP incidents
-
Think twice. Press once!
On a DP equipment class 2 supply vessel engaged in drilling, an incident occurred due to lack of operational knowledge
DPE 01/26
11 May 2026
Incident
-
Network issues, not a thing of the past
A DP equipment class 3 vessel was engaged in saturation diving activities, with two divers in the water when this DP incident occurred.
DPE 01/26
11 May 2026
Incident
-
All swept up
A DP equipment class 2 vessel was engaged in rock placement operations, within close proximity to a structure, when this event occurred.
DPE 01/26
11 May 2026
Undesired event
-
Hybrid system won't accept load
A DP equipment class 2 vessel was engaged in operations whilst holding position on auto DP, when this undesired event occurred
DPE 01/26
11 May 2026
Undesired event
-
DP drill scenario – Loss of main DP system UPS
The objective of this scenario is to identify risks and impacts of losing the main DP system uninterruptible power supply, possibilities to reduce that risk and suitable actions to be taken if such an occurrence happened.
DPE 01/26
11 May 2026
Drill Scenario
The case studies and observations above have been compiled from information received by IMCA. All vessel, client, and operational data has been removed from the narrative to ensure anonymity. Case studies are not intended as guidance on the safe conduct of operations, but rather to assist vessel managers, DP operators, and technical crew.
IMCA makes every effort to ensure both the accuracy and reliability of the information, but it is not liable for any guidance and/or recommendation and/or statement herein contained.
Any queries should be directed to DP team at IMCA. Share your DP incidents with IMCA online. Sign-up to receive DP event bulletins straight to your email.