- Discover how we are helping Members reduce emissions: Explore the ProjectGHG hub now.
- Join the global DP Community at the IMCA DP Conference in Amsterdam. 21 and 22 May. Book now
- Register your interest for the IMCA Global Summit 2024. 3-4 December, Utrecht, Netherlands.
- Now booking. Underwater Ship Husbandry Seminar. 10 October 2024, Singapore.
Lifting incident
An incident has been drawn to IMCA’s attention in which a load was being moved from deck to engine room on a vessel at sea. The crated load slipped from its slings and fell to the deck in the engine room below. There were no injuries. The incident occurred during daylight at sea. The vessel was underway, manoeuvring, in a sheltered bay awaiting wind speed to drop.
The operation of lowering the crate into the engine room through one of the engine room hatches had been discussed with those to be involved, about and hour or two earlier, at the daily work planning and safety meeting, but not documented, nor had a formal risk assessment or toolbox talk been carried out.
The seaman in charge of the operation contacted the Third Engineer to inform him that the lift would be coming down into the engine room. The Third Engineer sent an engine room assistant (ERA) to stand by to receive the load.
The weather situation was that the wind was at 30 knots, with a combined sea/swell reported as on the bow at Beaufort 4 (1.75 metres). The vessel was reported to be rolling approximately 1 to 2 degrees.
The lift team on deck comprised three deck personnel, one of whom acted as signalman, one as crane operator and one held a tagline.
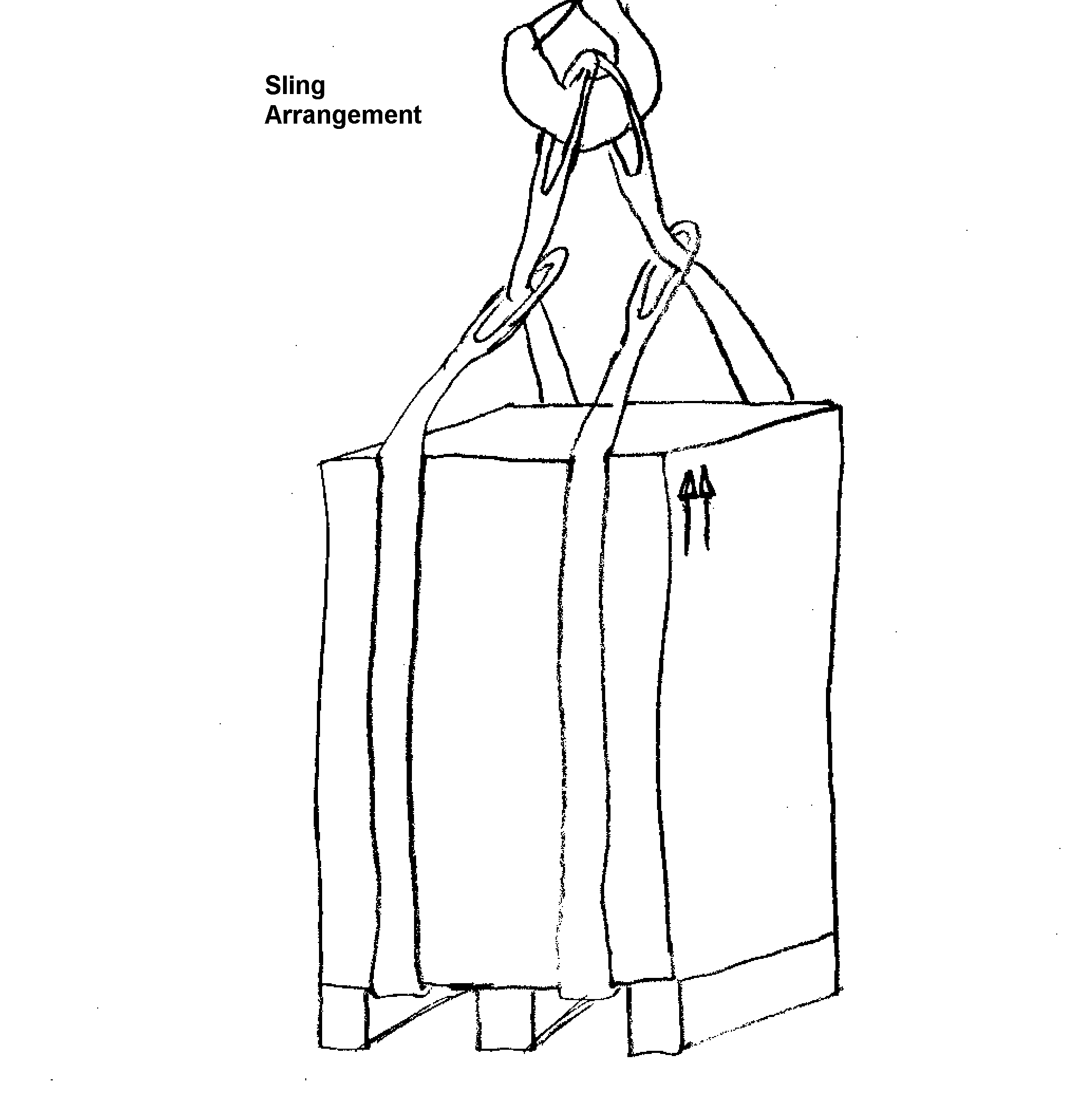
The aft port stores crane was utilised, lifting the crate from the port side towards and into the port side engine room stores hatch located inboard from the crane. The crate was secured to the crane using two slings rigged as chokers (see sketch below). There was a single tagline in use and the crane operator and signalman were in full view of each other throughout the operation.
The seamen involved were unaware of the contents of the crate. There were no officers present during the actual lifting operation.
The crate was secured to the crane hook using two 20 ft straps, described to be of SWL 8250 lbs when used as choker. The crane operator proceeded to lift the crate, holding it suspended for 20-30 seconds to ensure it was balanced properly. The crane operator received instruction from the seaman acting as a signalman while the other seaman controlled the tagline. An ERA was stationed in the engine room at the workshop deck preparing to receive the crate onto this deck. The crane operator proceeded to swing the lift inboard over the port hatch and began lowering the crate into the engine room.
All personnel noted that the lift was swaying slightly due to vessel movement, but no more than they had experienced with previous similar lifting operations. As the lift came horizontal with the ducting immediately below the coaming/deckhead the vessel experienced a larger roll and the crate swung to port and made contact with the ductwork. The signalman both signalled and verbally told the crane operator to stop lowering, which he did. The crate suddenly tipped to one side and the lifting sling on the high side of the crate slipped off, resulting in the crate tipping suddenly and falling to the deck below.
When the crate landed on the deck it broke open and the contents, an electrical high voltage circuit breaker weighing 250 kg., was damaged. There were no injuries, but the damaged circuit breaker had to be taken ashore to ascertain and repair the extent of damage incurred.
The company instigated an investigation which revealed to them that the immediate cause(s) of the accident were:
- failure to check and secure the contents of the load – although the piece of equipment had been transported to the vessel in a crated condition, the contents of the crate were not checked prior to lifting to ensure that no shifting had occurred which might lead to unbalancing the load;
- improper slinging, no method of preventing the slings from slipping – the crate measured 50″ L x 35″ W x 54″ H so it was a very high load, subsequently likely to be more subject to tipping/tilting if not balanced and rigged properly. The choking method was used to lift the crate, but there were no securing points to prevent the slings from slipping off if the load did become unbalanced;
- susceptibility to vessel motion – the motion of the vessel was not considered as a deterrent to performing the operation. The effect of a suspended load being much more susceptible to vessel motion was not recognised.
Root causes were found to be:
- Although those involved had crane operator familiarisation training, this needed to be supplemented by further computer based or practical training;
- Higher level of supervision of the lift should have been implemented;
- Company policy on lifting operations needed significant improvement. Risk assessment and permit to work procedures existed, but no formal lifting operations procedures;
- No formal risk assessment was conducted. Although a review of the task was conducted, there was no follow up risk assessment or toolbox talk;
- The lift was considered to be ‘routine’ in nature with a failure to appreciate the endemic risks;
- No recognition of the effects of the vessel’s motion, particularly on this load where the cargo had resultantly moved inside the crate;
- No check of the security of the load inside the crate;
- The vessel had performed numerous similar operations in the past without incident hence leading to a ‘routine’ job’ mentality by all involved.
It was also noted that:
- no notification was given to all engine room personnel that a heavy lift was being conducted overhead;
- there was a need for established lifting procedures, especially when negotiating areas like the engine room access hatch.
The following recommendations were made:
- As failure to conduct/review a formal risk assessment prior to the lifting operation led to this incident, it was recommended that a formal risk assessment is to be conducted for all lifting operations;
- Lifting operations to be supervised by a responsible officer;
- Updated crane operations training to be provided for all personnel normally involved in lifting operations;
- Rigging training should be investigated for key personnel;
- Company investigation report to be sent to other company vessel’s and industry;
- Method of incident investigation to be publicised;
- Awareness of benefits of risk assessment highlighted for all tasks, ‘routine’ or otherwise;
- Company investigation to be carried out regarding its training programmes;
- Training modified to include lifting operations and to include deck and engine room ratings;
- Paint marking and safety barriers to lift landing zone areas to be improved;
- Investigation to be carried out regarding improved ways of caging lifts to prevent loss by inadequate slinging;
- Formal supervised risk assessment to be conducted for all lifting operations;
- Appropriate and up to date crane operations training to be provided for all personnel normally involved in lifting operations.
Members can note that had guidance provided inGuidelines for lifting operations been followed, the incident should not have occurred.




Safety Event
Published: 25 February 2008
Download: ![]() IMCA SF 03/08
IMCA SF 03/08
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.